Radiographic assessment
Radiographic assessment and diagnosis of carious lesions in children
In both the primary and permanent dentition, radiography can be valuable in diagnosing the presence and extent of carious lesions and can be used for assessing caries progression. The broad contact points of the primary dentition make diagnosis of proximal caries difficult using visual examination alone. Although taking radiographs can be difficult, particularly with young or anxious children, bitewing radiographs can be an important adjunct to visual diagnosis of caries for children aged four and above. In view of the increased skin dosage, a dental panoramic radiograph should only be considered if there is a clear clinical indication, for example as part of a pre-general anaesthetic assessment.
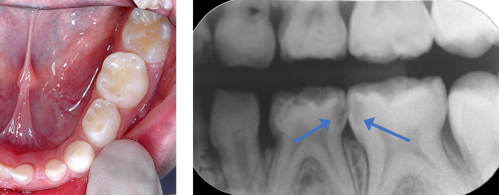
Image shows lower left primary molars with no cavitation (left) but enamel changes and advanced, proximal lesions are visible on the radiograph (right).
The frequency at which bitewing radiographs are taken should be based on an individual caries risk assessment and revised if the child’s risk of caries changes. Smaller films are available for use with children.27
For both primary and permanent teeth, accurate assessment of the extent of caries is essential to inform the management strategy. A judgement needs to be made about whether caries extends beyond the enamel-dentine junction into the outer, middle or inner third of dentine as illustrated below.

Image shows a diagrammatic illustration of outer, middle and inner thirds of dentine and dental pulp (dark grey).
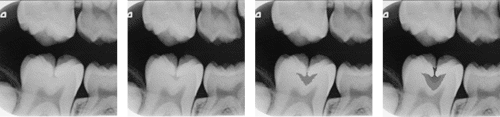
Images show (from left to right) enamel-dentine junction lesion, outer third lesion, middle third lesion, inner third lesion.
N.B. This radiograph has been digitally manipulated to illustrate the progression of an occlusal lesion.
To treatment plan management options for more advanced lesions (i.e. cavitation with visible dentine or widespread dentinal shadow; radiograph: inner third dentine) it is necessary to assess whether there is a clear band of normal looking dentine separating the carious lesion and the pulp. If a clear separation between caries and pulp cannot be seen, more invasive techniques are required.
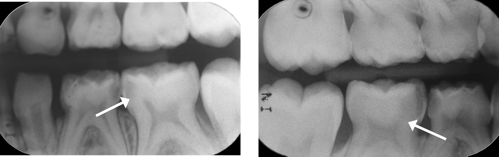
Radiographs show carious lesions with (left) and without (right) a clear band of normal dentine visible.
When a parent/carer expresses concern about exposing a child to X-rays, they can be reassured that the risks from dental radiography are very low and greatly outweighed by the diagnostic benefit. A bitewing radiograph is the equivalent of a few days' worth of background radiation.28
After clinical examination, if no previous radiographs have been taken or are available, consider taking bitewing radiographs to enable the extent of any caries to be accurately diagnosed.
If radiographs have been taken previously, take subsequent bitewing radiographs at the following intervals based on the child’s risk of developing caries (see Caries risk assessment).
- For children at increased risk of developing caries: 6-12 months.
- For all other children: 2 years.
These frequencies are based on recommendations by the Faculty of General Dental Practice (UK).27
Consider the use of orthodontic separators to assess for cavitation if enamel-only proximal lesions are identified.
When examining radiographs, be aware that some triangle-shaped radiolucencies seen on the mesial surface of maxillary second primary molars, and maxillary first permanent molars (e.g. just visible on maxillary E below) can be caused by the Cusp of Carabelli and may be mistaken for proximal caries.

Radiograph demonstrating a radiolucency caused by the Cusp of Carabelli
Such a radiolucency is more occlusally situated than is normal for a carious proximal lesion and there will be no opalescent white enamel (indicative of enamel/dentine caries) visible under the mesial marginal ridge and no radiolucency in the enamel.
Record all carious lesions, including white spot lesions.
Ensure the justification for taking radiographs is recorded in the patient’s notes as per radiation protection regulations.29
If there is a valid reason not to take radiographs as specified above (e.g. well-spaced dentition where posterior contacts are examinable and no other caries is visible or pre-co-operative child), record this in the patient’s notes.
Carious lesion management for primary and permanent teeth is discussed in Caries management in primary teeth and Caries management in permanent teeth respectively.
Taking bitewing radiographs with young children
The majority of young children are happy to have bitewing radiographs taken.30,31 If a child is anxious, consider a Systematic Desensitisation approach (see Behaviour management). Conventional film or digital plate radiographs may be used with smaller films/plates available for use with children.

Images show holder, films and digital plates (left); setting up the film holder (centre); applying the adhesive tabs (right).
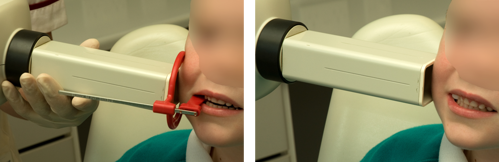
Images show 5-year-old boy having a bitewing radiograph taken using a Size 0 film with a film holder (left) and adhesive tab (right).
Use age-appropriate language. For example, explain to the child how much you would “like to have the pictures to help in looking after their teeth”.
Use film/plate holders where possible. If this is not possible, consider using adhesive tabs.