Assessing for pain and infection
Assessing for pain
Children are not always reliable in reporting pain, either because they have not yet developed the necessary communication skills or because they wish to avoid dental treatment. For example, an anxious child might not report an exfoliating tooth as painful, until reassured.
When obtaining a patient history, be aware that the child might not report pain reliably. Include input from the parent/carer as well as the child and ask about any problems with eating or drinking, changes to sleeping patterns and use of painkillers.
Advice on pain diagnosis and management is given in Pain or infection.
Assessing for dental abscess/infection in primary teeth
Dental abscess/infection can be difficult to diagnose because the clinical presentation can vary. Sinuses, if present, are not always obvious, but they are usually located on the non-attached mucosa adjacent to the attached mucosa. A slight cleft or notch may also be seen in the adjacent gingival margin.
It is unacceptable to ignore dental infection in the mouth, even if asymptomatic.34
Look for the following indicators of established dental infection (see images below):
- tenderness to percussion in a non-exfoliating tooth
- alveolar tenderness, sinus or swelling
- non-physiological mobility (compared with the healthy contralateral tooth) when the tooth is gently rocked bucco-lingually with the points of a pair of tweezers placed on the occlusal surface
- radiographic signs including inter-radicular radiolucency
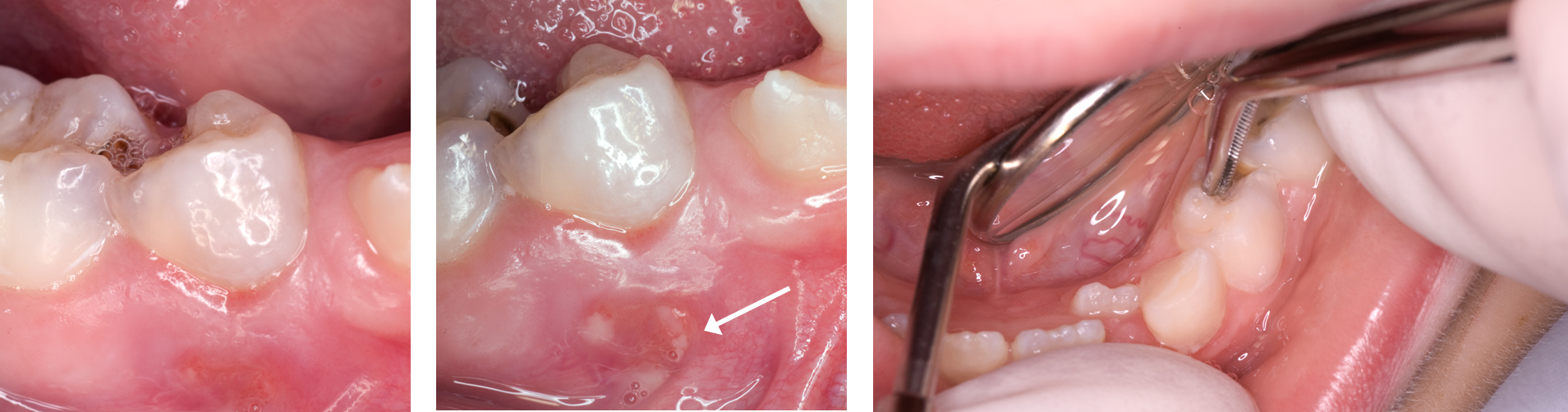
Images show: alveolar inflammation (left) that, on gentle palpation, releases infected material from a lower D (centre); assessing for increased, non-physiological mobility often associated with infection (right)
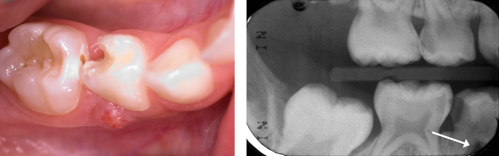
Images show a sinus (left) with associated inter-radicular radiolucency of lower D (right).
Advice on the management of infection is given in Pain or infection.