Primary molars - occlusal caries
Primary molar teeth with occlusal caries
Initial caries (occlusal)
Description: Visual diagnosis - teeth with noncavitated lesions (white spot lesions, discoloured or stained fissures; see Assessing carious lesions). There may be dentine shadowing or minimal cavitation where enamel is beginning to break down but no dentine is visible.
Radiographic diagnosis – caries may be visible in the outer third of dentine (see Assessing carious lesions).

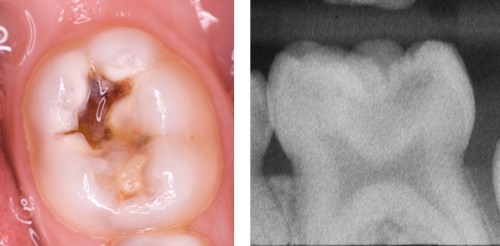
Photograph (left) and radiograph (right) showing a primary tooth with an initial occlusal carious lesion.
Aim: To use a minimally invasive approach to slow or arrest caries and reduce the risk of a tooth requiring a restoration.
There are alternative approaches for the management of an initial occlusal lesion in a primary tooth, the choice of which needs to be based on an assessment of the individual child.
Seal the lesion by placing a fissure sealant (see Sealant/infiltration). Alternatively, carry out site-specific prevention.
If a sealant is placed, monitor at each recall visit, top up the sealant if it is worn or fractured, and, if the lesion is progressing, adopt an alternative management strategy.
- Careful active surveillance, maintenance and repair of fissure sealants are essential to avoid the lesion progressing.
- Active surveillance involves checking the sealant visually and physically with a probe at each visit, and radiographically at risk-based intervals (see Assessing carious lesions).
If the child is unable to accept a resin sealant, consider placing a glass ionomer sealant using the press finger technique (see Glass ionomer sealant).
If the child is unable to accept any type of fissure sealant, consider sealing using the Hall Technique.
- Alternatively, if silver diamine fluoride (SDF) is already being used to treat advanced, cavitated lesions in that child, it is acceptable to also apply SDF to initial lesions, with the consent of the child and parent/carer (see Silver diamine fluoride).
Only continue with the selected approach if caries has arrested and there is no evidence of progression.
For these noncavitated lesions, fissure sealing is preferable. Resin fissure sealants are preferable to glass ionomer but the child’s cooperation may mean that a temporary glass ionomer sealant has to be used until the child is able to cope with a resin sealant (see Professionally-delivered interventions for application techniques).
Advanced caries (occlusal)
Description: Visual diagnosis – teeth with cavitation or dentine shadow and visible dentine.
Radiographic diagnosis - on a bitewing radiograph, these lesions are visible within dentine and may extend into the inner third. There should be a clear band of dentine visible that separates the carious lesion and the pulp (see Assessing carious lesions).
Photograph (left) and radiograph (right) showing a primary tooth with an advanced occlusal carious lesion.
Aim: To use a minimally invasive approach to slow or arrest caries, avoiding pulpal exposure and pain or infection before exfoliation.
If the caries is only present on the occlusal surface, carry out selective caries removal and restore using composite, resin modified glass ionomer, compomer or glass ionomer.
If the child is not cooperative enough for selective caries removal with a good adhesive restoration, seal in the caries using the Hall Technique.
If a proximal lesion is also present, seal using the Hall Technique.
If there is extensive cavitation, the tooth is not restorable or the child is not cooperative enough, consider a non-restorative cavity control approach, which may include the application of silver diamine fluoride.
The first choice of treatment for these lesions is selective caries removal and sealing with a restoration. The Hall Technique should only be used where the child is not cooperative enough for selective caries removal and for a good seal to be achieved with an adhesive restoration or if the proximal surface is affected.
Complete caries removal should not be carried out on these teeth because of the significantly higher risk of pulp exposure compared with carrying out selective caries removal.
Carious lesions which involve dentine can range from minimal to quite extensive. These lesions can still be managed minimally using a sealing in approach but care must be taken to detect lesions where there is no clear band of dentine visible radiographically that separates the pulp and the lesion. In these cases, the uncertain prognosis should be explained and treatment options discussed (see No clear separation).