Toothbrushing
Toothbrushing with fluoride toothpaste
Key recommendation
Encourage and support all children to brush their teeth, or to have their teeth brushed for them, at least twice a day using fluoride toothpaste, including recommending:
- the use of both an amount of toothpaste and a fluoride concentration appropriate for the child’s age and caries risk level
- supervised brushing until the child can brush their teeth effectively
- that children do not rinse their mouths after toothbrushing ("spit, don’t rinse")
(Strong recommendation; high certainty evidence)
Toothbrushing with fluoride toothpaste is one of the most effective methods for preventing caries. SIGN guideline 138 extensively reviewed the evidence related to toothbrushing including use of fluoride toothpaste, fluoride concentration, toothpaste composition, frequency and duration of brushing, age of commencement of brushing and toothbrushing practice.23
Advice on fluoride toothpaste use based on age and caries risk is summarised in the Fluoride toothpaste use based on age and caries risk figure below.
Further details about the development of the recommendations in this guidance can be found in Methodology.
Standard Prevention for all children
At least once a year, check that the child and/or parent/carer know how to brush effectively as follows:
Brush thoroughly twice daily, including last thing at night
- Brushing is best done in the morning and last thing at night before bed with nothing to eat or drink after brushing at night, apart from water. Brushing last thing at night is likely to be particularly effective due to reduced salivary flow and retention of fluoride in the mouth.
- In Scotland, toothbrushing at school or nursery as part of Childsmile is in addition to these two occasions.
Use the age-appropriate amount of toothpaste containing 1000 to 1500 ppm fluoride
- See Fluoride toothpaste use based on age and caries risk for details
"Spit, don't rinse"
- Children who spit out and do not rinse after brushing experience significantly less caries compared with those who rinse their mouth out with water after brushing.58,59
Supervise children until they can brush their teeth effectively (see Behaviour change)
- As younger children do not have the manual dexterity to brush their own teeth, the parent/carer must take responsibility.
Demonstrate brushing on the child (~3 minutes) annually.
- By modelling the desired behaviour, facilitating practice of the desired behaviour and giving reassurance that the behaviour is being done correctly, you can increase the child and/or parent/carer’s confidence and so the likelihood that the toothbrushing behaviour will be done at home.
Use action planning to encourage toothbrushing.
- For example, ask about daily routines and existing habits (e.g. getting changed in the morning and night, bedtime story) that could be used as a reminder to brush teeth immediately afterwards. Being very specific about what, when, and where something is done (action planning) increases the likelihood of it happening. The best way to establish a new habit (i.e. toothbrushing) is to attach it to something that is already a habit. For example, add toothbrushing to the evening bath time regime or just before the usual bed/story time.
Advise the parent/carer to start brushing as soon as the first primary tooth erupts.
Advise the parent/carer not to allow the child to eat or lick toothpaste.
Emphasise to teenagers the importance of regular brushing for oral health and the additional positive effect on the breath, appearance and general health.
Enhanced Prevention for children at increased risk of caries
At each recall visit provide Standard Prevention toothbrushing advice as detailed above.
Give hands-on brushing instruction (~3 minutes) to the child and parent/carer at each recall visit (see Behaviour change).
Consider providing additional preventive interventions depending on the child’s circumstances, for example:
- Recommend the use of 1350-1500 ppm fluoride toothpaste for children up to 10 years of age.
- Prescribe 2800 ppm fluoride toothpaste for children aged 10 - 16 years for a limited period (see SDCEP Drug Prescribing for Dentistry guidance for details). Regular review is required.57
Utilise any community/home support for toothbrushing that is available locally (e.g. health visitor, school nurse, Childsmile dental health support worker).
If at any time you have concerns about attendance, compliance or the child’s wellbeing, be prepared to provide additional support (see Providing additional support).
Fluoride toothpaste use based on age and caries risk
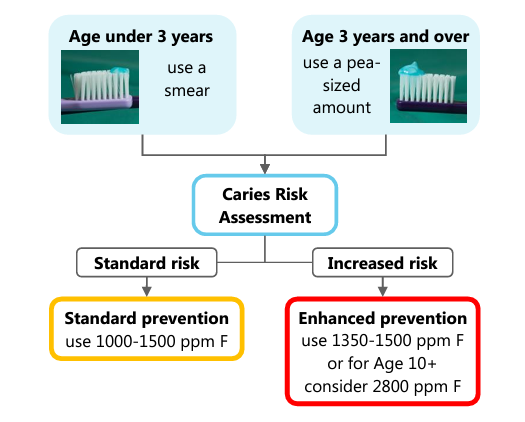
Based on Recommendations on the use of fluoride toothpaste and fluoride supplements in Scotland 2022.57
This technique incorporates both evidence-based actions for toothbrushing and behaviour change strategies (providing information, modelling, rehearsal, reinforcement, increasing control to build confidence and motivate, prompts, cues, incentives) to encourage regular effective toothbrushing.
Empathise with the parent/carer about how difficult it can be with small children to brush properly, but give advice (as described above) and reinforce the importance of following it.
Ask the child or parent/carer whether they would prefer to: (1) brush all surfaces of a section of the mouth, before moving on to the next section; or (2) the same surface of each complete arch, before moving onto the next surface (all cheek, all palate, all biting surfaces).
If the parent/carer is brushing the child’s teeth, ask them if they would prefer to stand behind their child, sit or kneel in front of the child.
Demonstrate the chosen technique on the child, and then encourage the child or parent/carer, or both, as appropriate for the age of the child, to show you.
- For example, the dental team member brushes one arch and then encourages the parent/carer to brush the other arch.
Instruct the use of a short, scrubbing motion. Teaching the child to recognise the ‘shh-shh’ sound of the correct brushing motion may be helpful.
Advise that it is likely to take at least two minutes brushing to clean all tooth surfaces and gums. Using a timer (e.g. watch or app) might help motivate the child.
Advise that after eating or drinking something acidic (e.g. fruit juice) it is preferable to wait at least 30 minutes before brushing.
When first or second molars are only partially erupted, show the child and parent/carer how brushing in line with the arch can miss the vulnerable occlusal surface of these teeth, and emphasise the need to brush the occlusal surface from the side of the mouth.

Image shows a child brushing occlusal tooth surfaces from the side of the mouth
Assess the likely benefits for the child of:
- Disclosing plaque at the brushing instruction visits and either recommending use of disclosing tablets or giving the parent/carer some to use at home.
- Providing toothbrushing charts on which the child or parent/carer can record each time the child’s teeth are brushed. This will act as a reminder about brushing frequency.
Consider providing a free toothbrush and free toothpaste to children at increased risk.
- In Scotland, Childsmile can supply practices with loose toothbrushes for demonstration and brush and toothpaste packs to give to children at increased caries risk.
Various resources to support parents, including a video about toothbrushing are available on the Childsmile website.